
( 6/7/22- I have attempted 3 times to add some thoughts to this original post. The first time I accidentally started it in a group rather than on my personal FB page which is where I intended to put it. Then two more attempts here within this blog, which is the best place to add a comment, resulted in shutting down of my WordPress altogether, wiping out the addendum twice. So, I’ve decided to let it just sit here as it is. ‘Nuff said.)
I was watching a lecture by physicist Shoshini Ghose on the new science of quantum computing, based on quantum physics. As she explained, quantum computing is altogether different from current computing technology based on combinations of binary “bits”….zeros or ones. In quantum computing a “quantum bit” has a more fluid, nonbinary identity. It can exist in a superposition, or a combination of zero and one, with some probability of being zero and some probability of being one. In other words, its identity is on a spectrum. For example, it could have a 70 percent chance of being zero and 30 percent chance of being one or 80-20 or 60-40. The possibilities are almost endless. The key idea here is that we have to give up on precise values of zero and one and allow for some uncertainty.
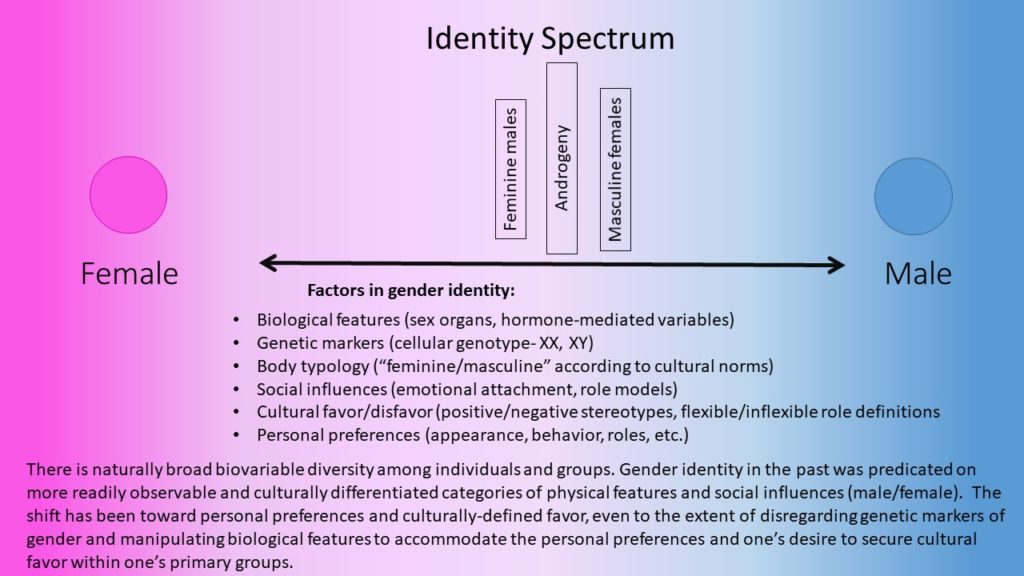
Dr. Ghose observed that a quantum computer creates fluid combinations in a quantum “bit” that cannot be predicted and, in the end, can move back to a position of zero or one from its mysterious and ever changing superposition…. like mixing two fluids, then unmixing them. It offers tremendous advantages for computer and internet security applications, maintaining the integrity of transactions and eliminating the risk of hacking. Her diagram of the simplicity of the quantum “spectrum” registered in my spirit with something I have been using to visualize the issue of gender identity in dealing with some individuals who have gender identity confusion.
The binary system (male/female) that we have historically used was based on simple observable biological features (and more recently on genetic markers for the same), as well as stereotypical assumptions about body typology and social behavior/roles and gender identification with same-gender parents by their children.
Recently, some government entities have added a new gender designation “X” (or “Other”) to the historical birth certificate designations of “male” and “female”, acquiescing to the liberal cultural demand to be free of such “either/or” designations in favor of the more individualistic preference to be whatever one chooses to be.
It remains to be seen if such individualized self-proclaimed gender statuses will be a temporary “fad” that will die out in 10-20 years or the beginning of a new standard for self-identity that transcends, and even dismisses, biology and genetics altogether. But, as in “quantum bits”, you can mix it anyway you choose, but in the end it’ll fall out one way or the- as zero or one – XX or XY. Unless genetic mutations create something other than XX or XY. I think, however, the broad, variable biodiverse spectrum that exists between the most extreme expressions of what is deemed “feminine” and the most extreme expressions of what is deemed “masculine” have always been around and will always be around. And the extremes themselves have always been more the exception than the rule.
I believe that God’s perfect will is expressed in the binary genetic state of male snd female. The fact of the brokenness of the the human condition has resulted in a number of genetic mutations that manifest a variety of symptoms and characteristics that belie the underlying brokenness. But compassion and understanding for those with such genetic mutations is necessary and healing, to whatever extent that can be accomplished, is appropriate. I think we have a lot to learn, understand and accomplish in the latter task.
from 2/27/21 by Chris Carey on FB
What determines gender? How do we know a person’s gender?
I am a physician who cared for patients for over 40 years. I am an OB/GYN, and have attended over 12,000 births. For years, the first thing the family wanted to know was “Is it a boy or a girl?” (Now they want to know with the first ultrasound!) But the question still remains – How do we know?
I have cared for many patients that the question could not be easily answered. Early in my career, I began to get referrals to see patients with gender “issues” – such as ambiguous genitalia, abnormal development of the genitalia, and gender dysphoria. I am a Christian by calling and am a Methodist by choice. The Wesleyan Quadrilateral resonates with me. When I was first deciding how much and what kind of treatments I could give, I struggled with doing the right thing. I will discuss how I came to the decision that I would treat gender issue, and how I reconciled my decision and calling with my faith.
I would like to explain a little about how the “usual” process occurs, and how it may not occur in the “usual” way. Then I will discuss what gender means. These discussions will of necessity be brief and incomplete. They are limited by my understanding, and God is not limited by my understanding.
The process of gender determination begins with the chromosomes. Typically a fetus gets an X chromosome from the mother and either and X or Y from the father. If there is an XY genotype, the fetus develops as a male. If there is an XX, the fetus develops as a female.
A developing embryo initially has undifferentiated gonads that can form either ovaries or testes and has precursors for both male and female internal genitalia (the Wolffian and Mullerian ducts). The external genitalia have precursors for both male and female genitalia (the genital tubercle). There is a region on the Y chromosome called SRY, (Sex Determining Region Y), that codes for a protein called the HY Antigen. If it is present, testes develop. The testes make testosterone and an anti-Muellerian hormone (AMH). Testosterone causes the Wolffian ducts to grow and form internal male genitalia, and AMH prevents the development of internal female genitalia. Testosterone causes the external genitalia to form a penis and scrotum, and the testes descend into the scrotum.
The usual female process is that in the absence of the SRY and HY Antigen, ovaries develop. The Wolffian ducts do not develop, and the Mullerian ducts form the fallopian tubes, uterus and upper third of the vagina. The external genitalia form the clitoris, labia and lower two thirds of the vagina.
Except, it does not always happen that way. About 1/500 liveborn infants are neither XX nor XY. XO, XYY, XXY and other combinations all occur. XO commonly miscarry but may appear to be normal female at birth. The ovaries do not develop normally, and do not produce estrogen at puberty, so secondary sex characteristics do not develop. XXY may appear to be normal male at birth, and may have infertility, delayed or absent puberty, or breast development, or not have any symptoms. XYY males may be larger and more aggressive, or may not show any symptoms.
The SRY gene can be present on an X chromosome. This leads to “XX males”, who may have testes. normal male internal and external genitalia. The SRY gene can be absent or non functional in an XY conception, leading to female internal and external genitalia and “streak gonads”.
There may not be androgen receptors present on cells in an XY fetus (androgen insensitivity syndrome, AIS). If complete, the person has normal female external genitalia and lower 2/3 of the vagina and develops normal female secondary sex characteristics at puberty, but the uterus and tubes do not develop. In incomplete androgen insensitivity, the person may have some varying degrees of ambiguous external genitalia. An XX fetus with Mullerian agenesis will not have development of the Mullerian ducts, and not have a uterus, fallopian tubes or upper vagina. These two conditions may present with identical symptoms, and usually identify as female.
An XX fetus may have some other source of androgen, either from adrenal hyperplasia or another source. They may develop ambiguous external genitalia. An XY fetus may not produce anti Muellarian hormone, and develop a uterus (often in the inguinal canal). There are other rare syndromes that can lead to different abnormalities of gender development.
So although chromosomes, internal, and external genitalia all play roles in determining a person’s gender, none of them are the sole determinant of “biologic” gender. There are additional determinants of gender like roles and behaviors. How do men and women act, and dress, and present themselves? Much of gender behavior is learned, and gender roles are learned. So we may identify gender by how people act and look. We treat people differently based on our perception of their gender – and on our perception of our own gender. People identify themselves as male or female -or they don’t. We identify other people as male or female – or we don’t. We are often very uncomfortable if we cannot assign a gender to someone – even if they are a disembodied voice on the phone, or a generated voice in our computer, phone, or GPS.
Differences from the usual process are not uncommon. About 1/500 live births are neither XX nor XY. Androgen insensitivity occurs in about 1/20,000 XY live births. Mullerian agenesis occurs in about 1/4500 XX births. Ambiguous genitalia occur in about 1/4500 live births. Gender dysphoria occurs in an estimated 1/300 people. As many as 1% of people do not fit into the “usual” development, although some estimates are higher than that. The term “intersex” is often used to describe persons with ambiguous genitalia, and may be used to include anyone who is not XY male or XX female.
But how do we know our own gender? It is clearly not all learned. People begin to identify as male or female by age three, before they understand anything about the process, or their chromosomes, or genitalia. You cannot “teach” a child to be the “opposite” gender. There is something in them that “knows” what they are. Infants with ambiguous genitalia who are assigned the “wrong” gender at birth often do not accept their gender assignment as they grow up, even if they do not know what happened to them.
We tend to love other people based on their gender. We may love people of the opposite gender, or the same gender – or both.
What is missing from any aspect of gender development and identity is personal choice. No one chooses their chromosomes, or how their internal or external genitalia develop, or what they are taught as children about gender – or what they feel they are, or whether they are gay or not.
Why would God choose to create people in all of these ways? How should we as Christians relate? As a physician, how should I treat these patients? I believe in the Wesleyan Quadrilateral – scripture, tradition, reason, and experience, and have used these principles to guide my choices.
The scriptures tell us that we are all made in God’s image. Gen 1:26 Then God said, “Let us make mankind in our image. Genesis 5 1-2 : When God created mankind, he made them in the likeness of God. He created them male and female and blessed them. And he named them “Mankind” when they were created. NIV. Jesus tells us that God made us by intent – John 9:1-3. 1As he went along, he saw a man blind from birth. 2His disciples asked him, “Rabbi, who sinned, this man or his parents, that he was born blind?” 3″Neither this man nor his parents sinned,” said Jesus, “but this happened so that the works of God might be displayed in him. Jesus then healed his blindness. The scriptures tell us that we should help and accept those who are different from birth, including “eunuchs”. Matthew 19:11-12 Jesus replied, “Not everyone can accept this word, but only those to whom it has been given. For there are eunuchs who were born that way, and there are eunuchs who have been made eunuchs by others-and there are those who choose to live like eunuchs for the sake of the kingdom of heaven. The one who can accept this should accept it.” NIV. Man made eunuchs often had their testes and penis removed, and those who were “born that way” were known to exist.
My experience with patients has taught me that we are all “born that way” – the way we are. I am arrogant and egotistical, and I knew I could use medicine and surgery to “correct” ambiguous genitalia, or induce secondary sex characteristics, or perform gender confirmation surgery – creating a vagina, clitoris and labia from a penis and a scrotum. I was presented with patients who wanted and needed these procedures. Was I called to care for them, or was it my ego telling me that I had the power to go against God’s will? With the help of a wise and compassionate pastor, my spiritual journey led me to decide that I could and should treat these patients as needed. I believe that it was God’s plan for me to do so. God is not limited by my understanding, and He rarely shares his long term goals or strategy with me. Why me? I do not know, but I can accept it.
I believe that everyone is of sacred worth and is made in God’s image. I also believe that Jesus healed people wo were “born that way” and so God intended us to treat people with birth conditions if we can. There is no treatment for homosexuality, but there can be treatment for people who are struggling with their orientation, and how to live with who they are. Neither they nor their parents sinned. There is no treatment for being trans gendered, but the gender dysphoria – the pain of being trans, of waking up every morning in a body that does not fit your self, can and should be treated. Treatments depend on the individual patient’s needs and wants.
But to dismissively say that there are two genders, male and female, and science proves it – is simply wrong. To tell a girl with androgen insensitivity that she cannot play basketball or run track because she is XY and has testosterone is profoundly ignorant – and cruel. To tell a XX male that he is a woman is ignorant and cruel. To tell a gay or trans person that they should deny who they are, or that the way they are is a sin, is wrong and denies God’s will and power. We are all made in God’s image, for His purpose. God calls us to love everyone, even when we do not understand His purpose. Everyone was put here to fulfil God’s plan and will and feel His love. Our role is to love and help those in need, even if we do not understand.
You may note that I refer to God as male. He shows himself to me in that way because He know that is what I can understand. I am a Muscogee, and sometimes God shows himself to me as a bear – because he knows (hopes?) that I will listen then, and He may need to maul me to get my attention. Often he is the still small voice that spoke to Elijah in the cave, and speaks to me in that way. None of us can understand God in his glory, and we have to listen and understand as best we can in the way that we can.